
Unit 13
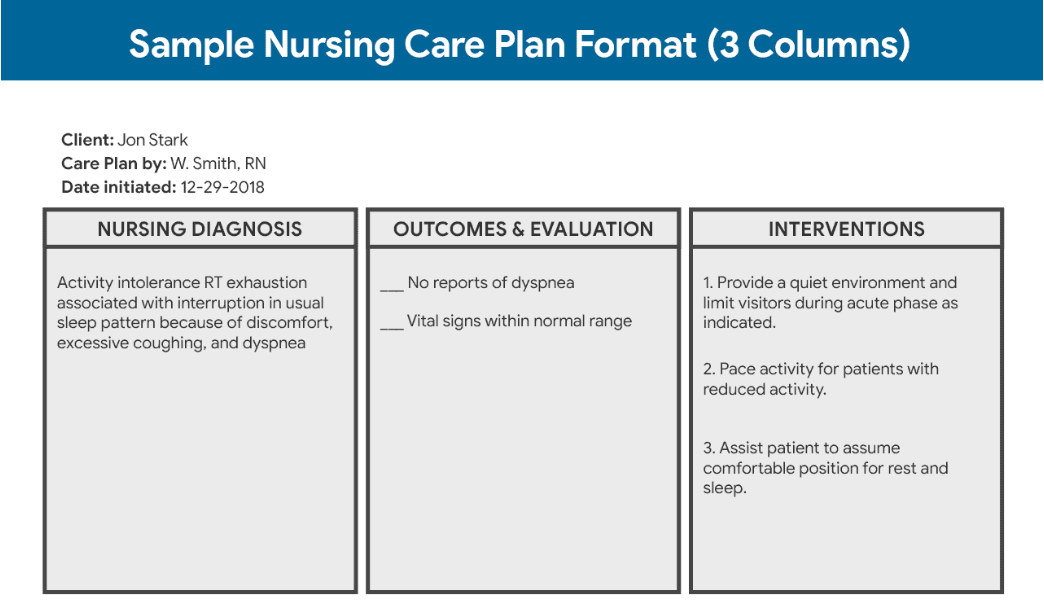
The resident's care plan
The resident's care plan is a legal document required by OBRA 87 stating that every resident is to have a plan of care developed for each resident with the involvement of the resident/family. A care plan is a living on-going document meaning it is to be changed to reflect how the residents is at that moment. Care plans are done on a rotating basis depending on the payor source, and can be every 7 days for a short Medicare stay to as long as every 90 days. Care plans can be updated between scheduled dates as well.
The care plan is a way for interdisciplinary team members to come together and review and create a plan of care designed specific for each resident.
The care plan team usually consists of:
Director of Nursing (DON) MDS coordinator (a nurse that specializes in assessments, documentation and care plans). Restorative Aide, Therapies (OT, PT, ST) Dietary Manager or Registered Dietitian, Activity Director, Social services, the physician or their proxy and most importantly, the resident and/ or family members. C.N.As and other staff members fill out documentation and give input as well.
The documentation the C.N.A completes every shift for the residents being care planned and is used for guidance for decision making.
The focus of meeting to create the care plans is to ensure quality of consistent care and to promote the quality of the resident's life. The care plan must have the goals of the resident not the staff of the LTC community.
When the members of the care plan team come together they follow the nursing process to develop the care plan.
The Nursing Process & The CNA
The nursing process is divided into five steps, however the state curriculum does not include diagnosis so for this class we will not include it in the quiz and limit it to 4 steps.
Assessment
Planning
Intervention/Implementation
Evaluation
1. The Assessment - The resident is assessed by an RN, all documentation and the resident's history is taken into consideration the nurse also performs a physical and mental exam that is according to the level of training. The resident is asked several questions regarding depression and how they feel they are doing. Once all the assessments are complete, the nurse inputs the information in a form called an MDS (Minimum Data Set). The MDS is then sent to the state so the state can determine the level of care the individual needs, and this is what will determine reimbursement if the resident is on Medicaid or Medicare. The MDS also analyzes the results of the assessments and creates a list of problems and risk factors from which the nurse can create their care plan. For example: Because the MDS reflects that Mr. Greene needs 2 person transfers, is incontinent, and is diabetic, the MDS may list "Risk for skin breakdown". The nurse would then develop a care plan to address this risk.
2. Planning - Once the assessment is completed and issues, diagnosis, problems are identified it is time to make a plan to address every single one of the identified issues. Part of the planning is setting goals. The goals absolutely must be the residents goals and not the goals that others might think the resident should want. Without the goals, planning really does not matter.
Example: Mr. Greene, a 95 year old male is a new admission to your LTC community. Mr. Greene had lived alone in his apartment with his cat before falling, hitting his head resulting in a large subdural hematoma which left him with a huge self care deficit and pain.
Scenario #1 - Mr. Greene states his goal is to take his pain medications and keep as comfortable as possible, no further surgeries or heroic measures to stay alive, he is content and ready to pass on.
Scenario #2 - Mr. Greene states he is determined to work as hard as he can in PT/OT to rehabilitate and get back to his apartment and his little cat.
Do you see how the plan really depends upon the resident's own goals? Depending which way Mr. Greene chose, the plan would vary greatly.
Plans include showering, exercising, food, fluid choices and plans, therapies, medications, socialization plans and much much more.
3. Intervention/Implementation - This is where it is documented who is responsible for each of the plans...who does what and when. This supports accountability.
4. Evaluation - Every time the care plan team meets every item in the care plan is evaluated. Was it done, did it work, has the resident changed and we need a new goal or plan? Adjustments are made and a new plan of care is formed.
The nursing process is not just for care plans it is used for every day problem solving. Now, you can use it as well.