Unit 6
Range of Motion Exercises
Lost mobility is a possibility in residents who do not regularly participate in physical activity or exercise, including ROM (Range of Motion) exercises. Nursing assistants often assist with ROM, stretching residents' muscles and gently moving the joints in order to keep them supple and flexible. As residents become less and less mobile, they may stop moving their joint as much which can lead to a permanent shortening or hardening of soft tissue resulting in deformity or rigidity of joints (frozen in a flexed position) called contractures.
Range of motion exercises are performed by putting each joint through ten reps in every direction that joint can move. For example, the wrist can flex and extend, but it can also move in a circular pattern. If the resident is able to perform the reps independently they are actively participating so the exercise is considered active range of motion (AROM). If the staff must move the joint for them, the resident is passively participating so it is considered passive range of motion (PROM).
Why is mobility so important?
One obvious benefit that outweighs them all is the ability to be independent. The more mobile someone is, the more independent they can be, which leads to a greater sense of accomplishment, self-esteem, and overall well-being. Ambulation (walking) alone improves their health by all of the following and more:
Stimulates peristalsis (muscle action that keeps food moving in the right direction) which improves appetite and prevents constipation
Improves blood circulation which can prevent edema (swelling) and blood clots
Prevents osteoporosis, a condition where bones become porous and brittle and break easily
Helps prevent pain from osteoarthritis (inflammation in the joints from normal wear and tear)
Prevents atrophy, the shrinking of muscle mass due to protein deficiency and decreased exercise
Cerebral vascular accident (CVA)
A CVA, or stroke, can affect any area of the brain. A stroke is what we call it when a blood vessel in the brain is either clogged with a blood clot or sometimes, it bursts and there is a bleed. If either of these things happens the tissue that blood vessels fed will die from lack of oxygen causing brain damage. The lasting effects of a stroke are evident by where the brain death occurred in the brain. If damage occurs in the language center then the resident may have difficulty communicating; if it occurs in the occipital lobe it will affect the vision; or if it occurs in the frontal lobe it will affect their personality and cognition. If a stroke occurs in the mobility centers of the brain it can cause weakness or complete paralysis. Since the right half of the brain controls the left half of the body and the right half of the brain controls the left half of the body independently, the weakness or paralysis only occurs on one half of the body- the opposite side of where the stroke occurred, This is called hemiplegia. Hemi=half; like hemisphere and plegia=paralyzed, like paraplegia or quadriplegia. 70% of stroke victims end up requiring extensive care in a nursing home within one year.
CNA’s role in Mobility:
Encourage resident to participate with control and confidence
Prevent deterioration in condition
Provide Safety
Follow Care Plan
Body Mechanics
Body mechanics refers to the way you hold your body when you move around. Proper body mechanics help you avoid muscle fatigue and injuries as you walk, bend over, lift objects, or perform other activities of daily living. Think of body mechanics as good posture in motion.
How to use the body correctly when moving residents or objects
Use largest muscles
legs, squat down
bend at knees
back straight
raise straight up
no twisting or bending at waist
Use both arms
Stand erect, good posture
Keep object/resident as close as possible and at the level of your center of gravity
Face object/resident
Feet should be shoulder-width apart
Wear non-slip shoes
Use arms to support object
Push, pull, slide, roll instead of lifting
Use smooth, steady movements
Keep muscles strong.
General principles for lifting and moving a resident
You should understand how the resident may be moved, what he/she can do to assist, and mobility goals. Make sure to check the care plan or ask the nurse about the resident's mobility goals.
Weight bearing is an important concept to understand in regards to how much assistance a resident might need. If a resident is full weight bearing they can bear their own full weight. This means that when they stand up, transfer to a seat, or walk, no one has to help them support their weight, or use their own strength to help them manage the task. Weight bearing is not limited to just bearing weight on their legs either. It can refer to lifting an arm to get dressed, hand-over hand feeding, or even turning over in bed. If a resident is full weight bearing but requires assistance with a task, such as holding up their shirt while they slip their arms into the sleeves or perhaps walking with them with a gaitbelt, this is called limited assist. Limited assist only requires one person and no lifting or weight bearing by the staff is needed. If a resident requires the staff to lift or bear any of their weight for them, this is called extensive assist. If a resident requires a mechanical lift for transfers, the CNA has to help them to their feet and steady them before they can walk or pivot, or if the resident is unable to roll over on their side on their own they would be considered an extensive assist.
Key steps to remember when tranfering:
Check the resident's care plan before attempting any kind of care
CNA's should plan for help from other staff when moving a resident
Use mechanical lifting devices or other devices whenever possible.
Facilities may have implemented "no lift", "free lift", or "safe lift" policies which means that any lifting needed should be done by a mechanical lift and not the staff
Know how to use devices safely.
Work in coordination when lifting or moving resident with another person. "1-2-3"
Explain procedure to resident, give cues about what the resident can do to help.
Protect all tubing and dressings when moving resident.
Give most support to heaviest part of body. Keeping the heaviest load at your center of gravity (belly button)
Position resident so gravity can help with the move. (have the resident lean forward or raise the head of the bed (HOB) etc)
Take your time. Allow resident to maintain control. A resident may experience a period of dizziness when changing position so allow them to sit for a minute before standing if they have been laying in bed.
Observe and report resident's ability to participate in activity, and report any changes
Gait Belt
A gait belt is an assistive device which can be used to help safely transfer a person from a bed to a wheelchair, assist with sitting and standing, and help with walking around. It is secured around the waist to allow a caregiver to grasp the belt to assist in lifting or moving a person. When used properly, the belt protects the care recipient from falling and also protects the caregiver from injuring his or her back as they lift or move the care recipient. If a resident loses their balance and starts to fall it is important to understand that you can't usually stop the fall and may injury yourself if you try, but the gait belt should give you the ability slow their fall and possibly prevent their head from hitting the floor. In addition, the gait belt helps you to hold the bulk of the resident's weight at your center of gravity making the lift considerably easier and more comfortable for the resident.
A gait belt is usually 1-½ to 4 inches wide, and 54-60 inches long. The belt is made out of canvas, nylon, or leather with a buckle at one end.
Applying a Gait belt
Apply to resident’s waist
Check for tightness
Resident should have on non-slip shoes
Resident should put hands on forearm or elbow not on shoulders or neck
Report changes in mobility to nurse.
Alignment refers to how the head, shoulders, spine, hips, knees and ankles relate and line up with each other. Proper alignment of the body puts less stress on the spine and helps you have good posture. To keep proper alignment, avoid the following positions or movements: Having a slumped, head-forward posture.
Residents who are immobile may experience disuse osteoporosis, disuse atrophy, contractures, reduced skin turgor and skin breakdown.
The mentioned complications can be avoided when a patient is positioned to maintain a proper body alignment. Thus, joint contractures and deformities are prevented. Improper positioning of a resident can result in pressure ulcers which can develop in just 24 hours but requires months to heal. Since pressure ulcers develop when their weight compresses the skin between a bone and a hard surface for too long, it is essential that residents are repositioned at least every two hours and low pressure cushions are used in their wheelchairs and beds. Proper posture must be maintained as near as normal to an upright position if patients are immobile or confined to bed.
Body Alignment
Alignment is the correct positioning of the resident’s body
Correct positioning helps to prevent contractures and undue pressure
Posture changes with aging
Osteoporosis
Loss of balance
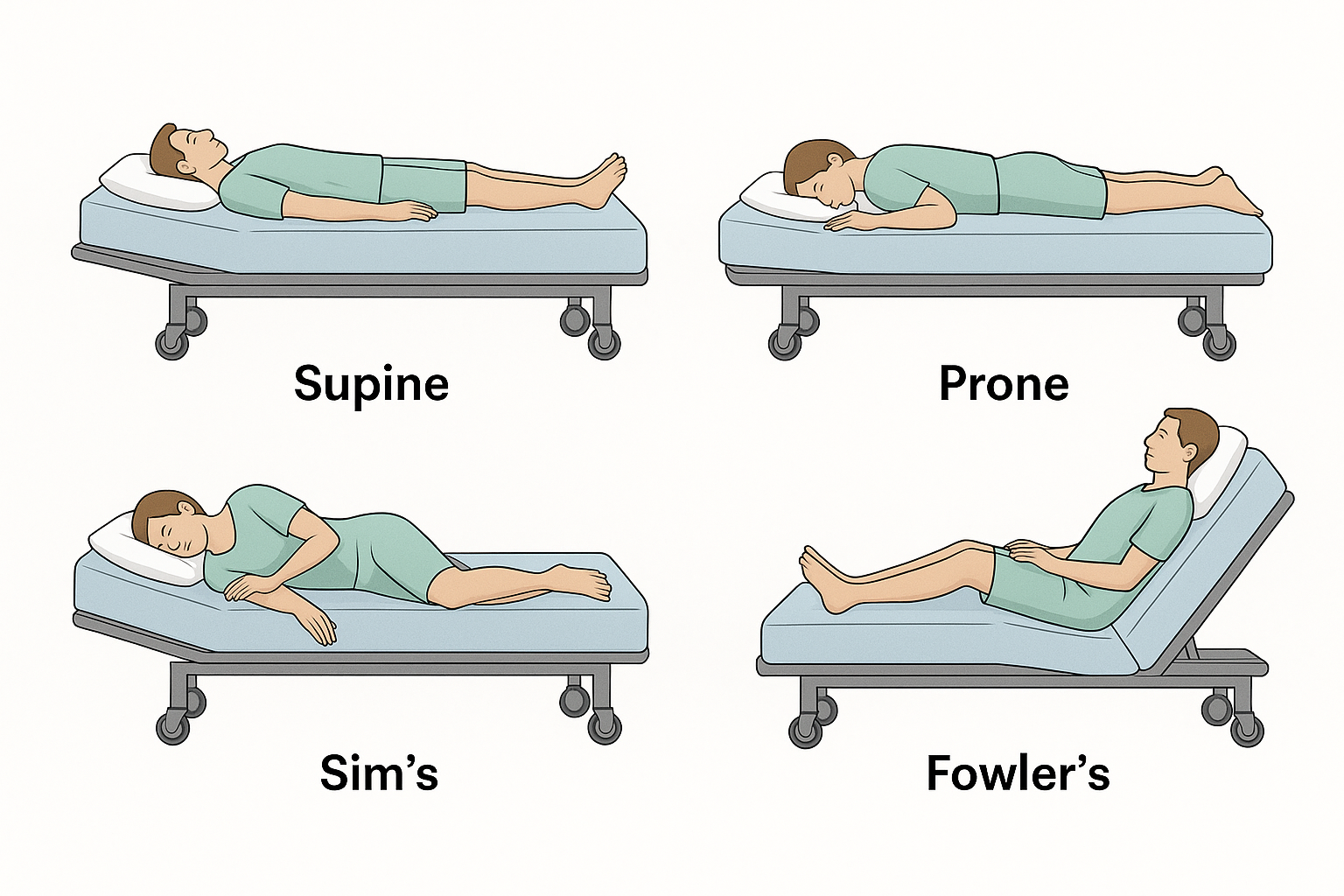
Positions:
Supine-(of a person) lying face upward.
Prone-lying flat, especially face downward.
Sim’s- lying on the left side, with right hip and knees bent.
Fowler's - A position in which the head of the bed is raised 30 to 90 degrees above the level, with the knees sometimes also elevated.
Alignment Devices:
Pillows
Foam Wedges
Trochanter Roll
Abduction splint
Palmar (Hand/wrist) Splint
Hand Roll
Foot Board
Assistive Devices: (Cane, Walker, Crutches)
Check Care plan for ambulation goals
Check Device to see that it is safe
Slip-Proof shoes
Transfer belt stand slightly behind and close to the resident’s side holding the center back of the belt.
Encourage to walk to activities
Encourage resident to walk with good posture
Observe and report resident’s activity and any sign of illness.
Wheelchair (w/c)
Understand mobility goals and follow the care plan
Positioning in w/c (hips/knees/ankles all at 90 degree angles)
Feet on footrest if not self propelled
Arms and elbows inside arm rest
Lap blanket when needed, if catheter bag is in use, ensure it is covered and secured below level of bladder under the w/c not touching the ground.
Moving- forward unless backing into an elevator or down a ramp or slope
Warn the resident before suddenly moving them
Set breaks when stationary or during a one person transfer
Low pressure cushion in seat
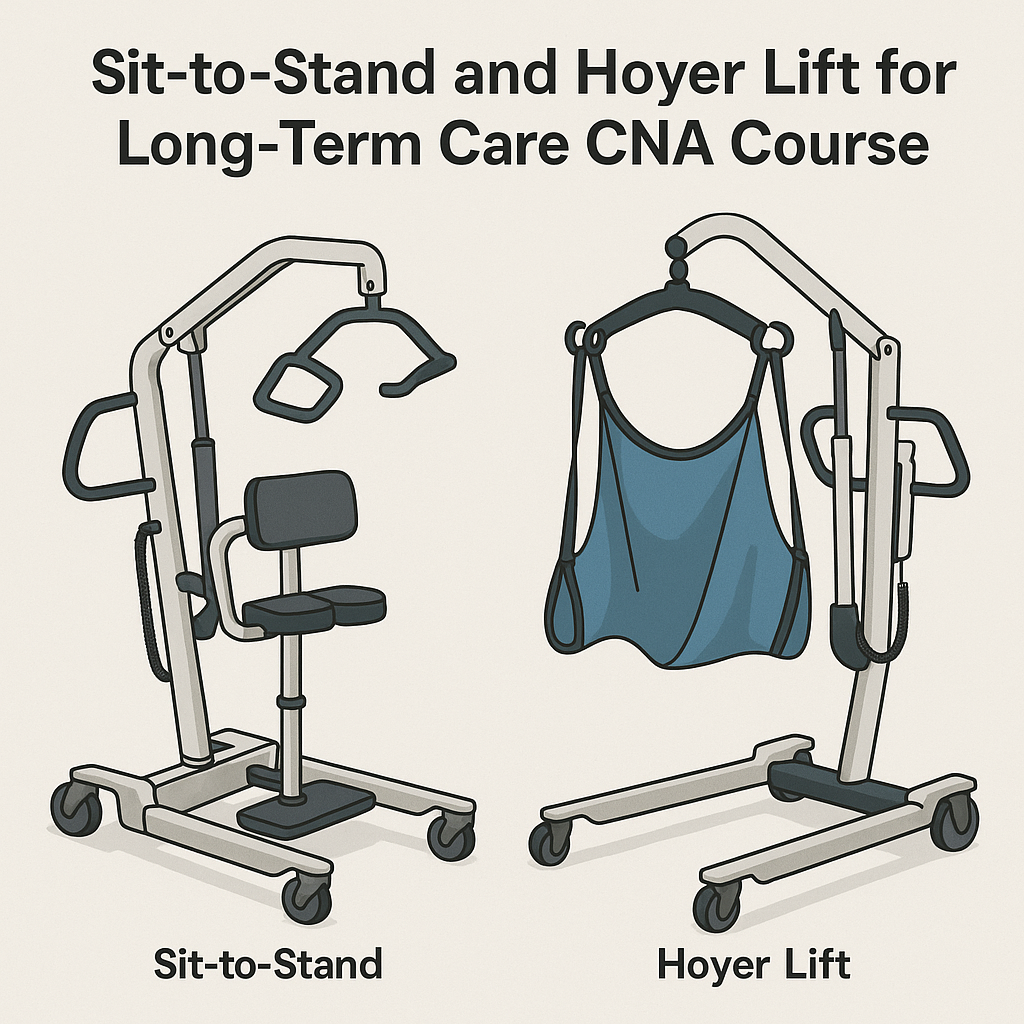
Mechanical lifts
Sit to stand lift
Total body lift (Hoyer)
Follow the policy of the LTC community regarding the number of staff that need to be present to use lifts. Two or more staff are required unless in a home care setting. You must be 18 to operate a lift and may only assist when under 18. Make sure you understand how to use the lift. When using lifts consider resident’s privacy and anxiety. Before using any lifts make sure all mechanical elements work properly and use brakes appropriately. Never use a sling that is fraying or ripped.