
Unit 15
Changes in the Muscular/Skeletal system in aging and steps the C.N.A can take to assist
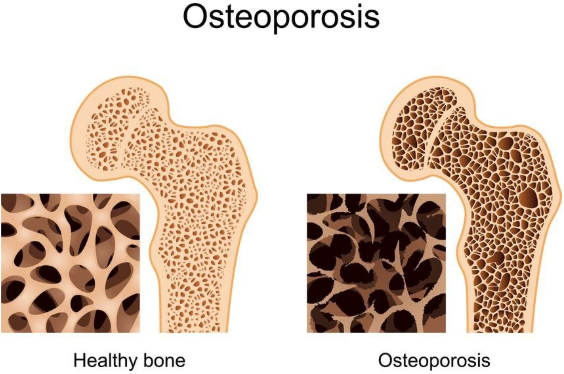
People lose bone mass or density as they age, especially women after menopause. The bones lose calcium and other minerals.
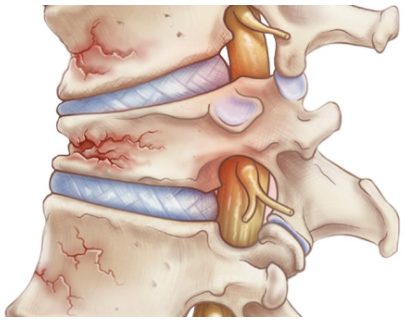
The spine is made up of bones called vertebrae. Between each bone is a disk, a gel-like cushion. With aging, the middle of the body becomes shorter as the disks gradually lose fluid and become thinner, this is why people shrink in height by up to 2 to 3 inches.
Vertebrae also lose some of their mineral content, making each bone thinner. The spinal column becomes curved and compressed. Bone spurs caused by aging and overall use of the spine may also form on the vertebrae.
The foot arches become less pronounced, contributing to a slight loss of height and foot pain that radiates up the leg to the hip.
The bones of the arms and legs are more brittle because of mineral loss, but they do not change length. This makes the arms and legs look longer when compared with the shortened trunk.
The joints become stiffer and less flexible. Fluid in the joints may decrease. The cartilage may begin to rub together and wear away. Minerals may deposit in and around some joints. This is common around the shoulder.
Hip and knee joints may begin to lose cartilage. The finger joints lose cartilage and the bones thicken slightly. Finger joint changes, most often bony swelling called osteophytes, are more common in women. These changes may be inherited.
Lean body mass decreases. This decrease is partly caused by a loss of muscle tissue called atrophy.
The muscle fibers shrink. Muscle tissue is replaced more slowly. Lost muscle tissue may be replaced with a tough fibrous tissue. This is most noticeable in the hands, which may look thin and bony.
Muscles are less toned and less able to contract because of changes in the muscle tissue and normal aging changes in the nervous system. Muscles may become rigid with age and may lose tone, even with regular exercise.
The Effect of these Changes
Osteoporosis can occur where the bones become more brittle and may break more easily.
Overall height decreases, mainly because the trunk and spine shorten.
Breakdown of the joints may lead to inflammation, pain, stiffness, and deformity. Joint changes affect almost all older people. These changes range from minor stiffness to severe arthritis.
The posture may become more stooped (bent). The knees and hips may become more flexed. The neck may tilt, and the shoulders may narrow while the pelvis becomes wider.
Movement slows and may become limited. The walking pattern (gait) becomes slower and shorter. Walking may become unsteady, and there is less arm swinging. Older people get tired more easily and have less energy.
Strength and endurance change. Loss of muscle mass reduces strength.
COMMON PROBLEMS
Osteoporosis is a common problem, especially for older women as the bones are weaker and thinner. Bones break more easily. When the bones in the vertebrae (back bone) become weak and full of microscopic holes from loss of minerals, they can fracture and can cause constant chronic pain and reduce mobility. These are called compression fractures of the spine.
Muscle weakness contributes to fatigue, weakness, and reduced activity tolerance. Joint problems ranging from mild stiffness to debilitating arthritis, such as degenerative joint disease also called osteoarthritis is very common.
The risk of injury increases because of changes in the gait (the way one walks-posture), instability, and loss of balance may lead to falls.
Some older people have reduced reflexes. This is most often caused by changes in the muscles and tendons, rather than changes in the nerves. Decreased knee jerk or ankle jerk reflexes can occur.
Involuntary movements (muscle tremors and fine movements are more common in the older person. Older people who are not active may have weakness or abnormal sensations.
People who are unable to move on their own, or who do not stretch their muscles with exercise, may develop contractures which is a permanent shortening of ligaments or tendons.

Steps to Assisting Residents with these Issues
Be patient and understanding - Many of these conditions result in pain and cause the resident to move much slower than you might think is necessary. Give the resident time to do things they can on their own, even if it takes longer. You may be very busy but this cannot be conveyed to the resident.
Protect from Falls - This can be a difficult balance between independence in resident rights and protecting them from injury. The focus must be on how to support the resident's free will and choices while preventing injury. Talk with the resident and come up with ideas and share these ideas with the care plan team. An example might be-"The resident does not like to use his walker when in his room as in going from easy chair to the toilet or bed". A compromise might be a cane to use while in the room as it is not as bulky and arrange the furniture for straighter paths and items to hold on to when walking.
Observe / Report Pain - Some elders are slow to complain about pain, but pain can be a sign of compression fractures or other injuries which need to be reported.
Reposition for comfort - Do not underestimate the difference you can make by using several pillow to off load painful areas so the resident can rest comfortably.
Splints, Braces, Hot and Cold Treatment - Generally, the resident cannot apply these alone and may forget or be worried to ask because you are busy, be mindful of these and take the initiative to apply.